
A combined Clinico Radiological case from Dr Joe Thomas (Rheumatologist)
This is a combined case with Dr Joe Thomas on a case of Polyarteritis Nodosa that presented with Myositis and Myopericarditis. Dr Thomas is a senior consultant Rheumatologist who is also joining us in presenting the Spine Arthropathy and Spondyloarthropathy course.
- 20-year-old student presented with polyarthritis.
- ESR 38, CRP 11, ANA(IF) speckled 2 +, ANA profile showed ds DNA 2 + and SCL 70 1+, dsDNA positive by elisa (461).
- Diagnosed as SLE and was on treatment with HCQS, steroids, methotrexate.
- Persistent joint pain with fever and rising inflammatory markers (ESR 90, CRP121) despite treatment.
- PET CT : Inflammatory arthritis with enthesitis.
- Managed with pulse steroid and rituximab 500mg.
![]()
- Readmitted in view of persistent fever and generalized myalgia in functional class 4.
- Inflammatory markers- ESR 120, CRP 201.
- Work up for infection and malignancy were negative (including bone marrow).
- Steroids and IVIG were started.
- Developed left lower limb numbness with gait abnormality and severe retrosternal chest pain.
![]()
- Admitted in ICU in view of severe chest pain (requiring opioids to control pain).
- Very high inflammatory markers, Trop I- 740.0 ng/L (N<9) and repeat work up for Lupus was negative.
- ECHOCARDIOGRAM: Global LV hypokinesia with severe left ventricular systolic dysfunction.
- Diagnosis at this stage was severe myopericarditis secondary to autoimmune disease.
![]()
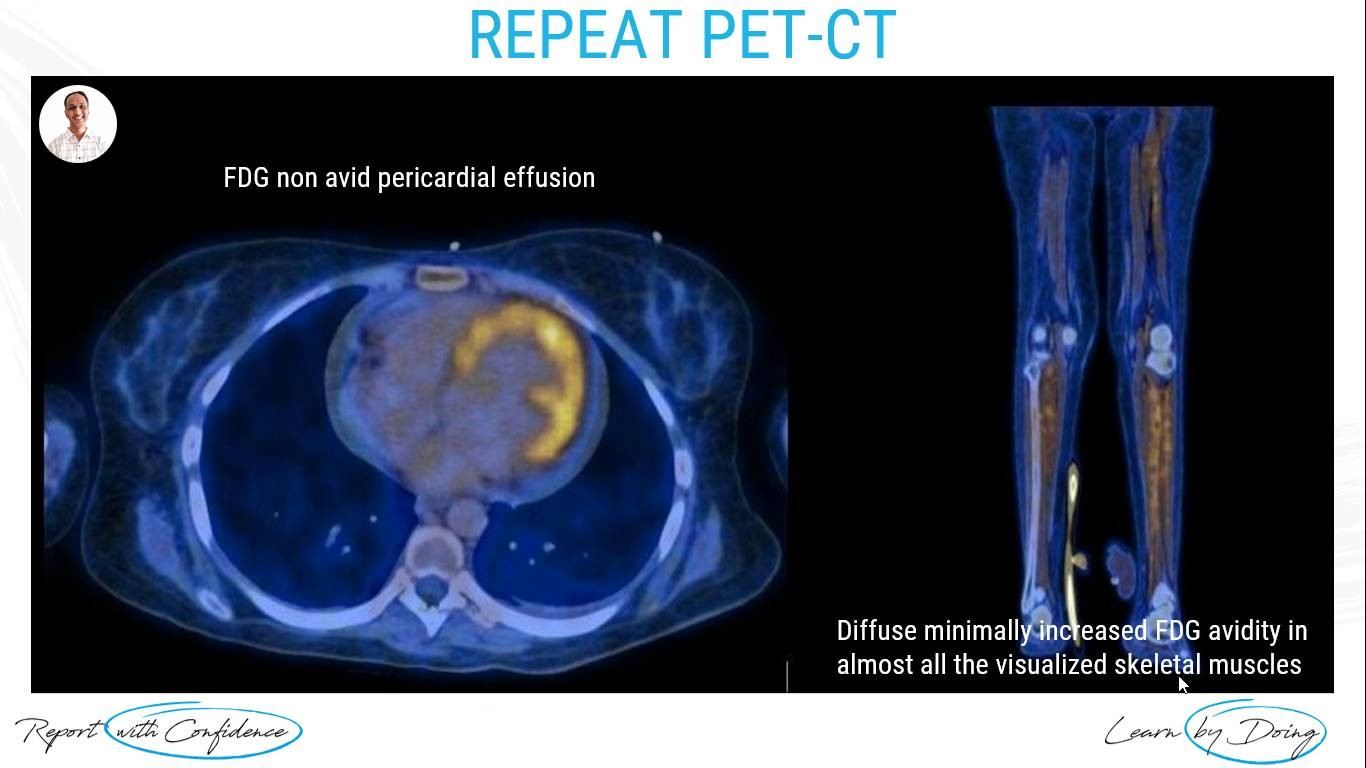
- FDG non avid pericardial effusion.
- Diffuse minimally increased FDG avidity in almost all the visualized skeletal muscles.
![]()
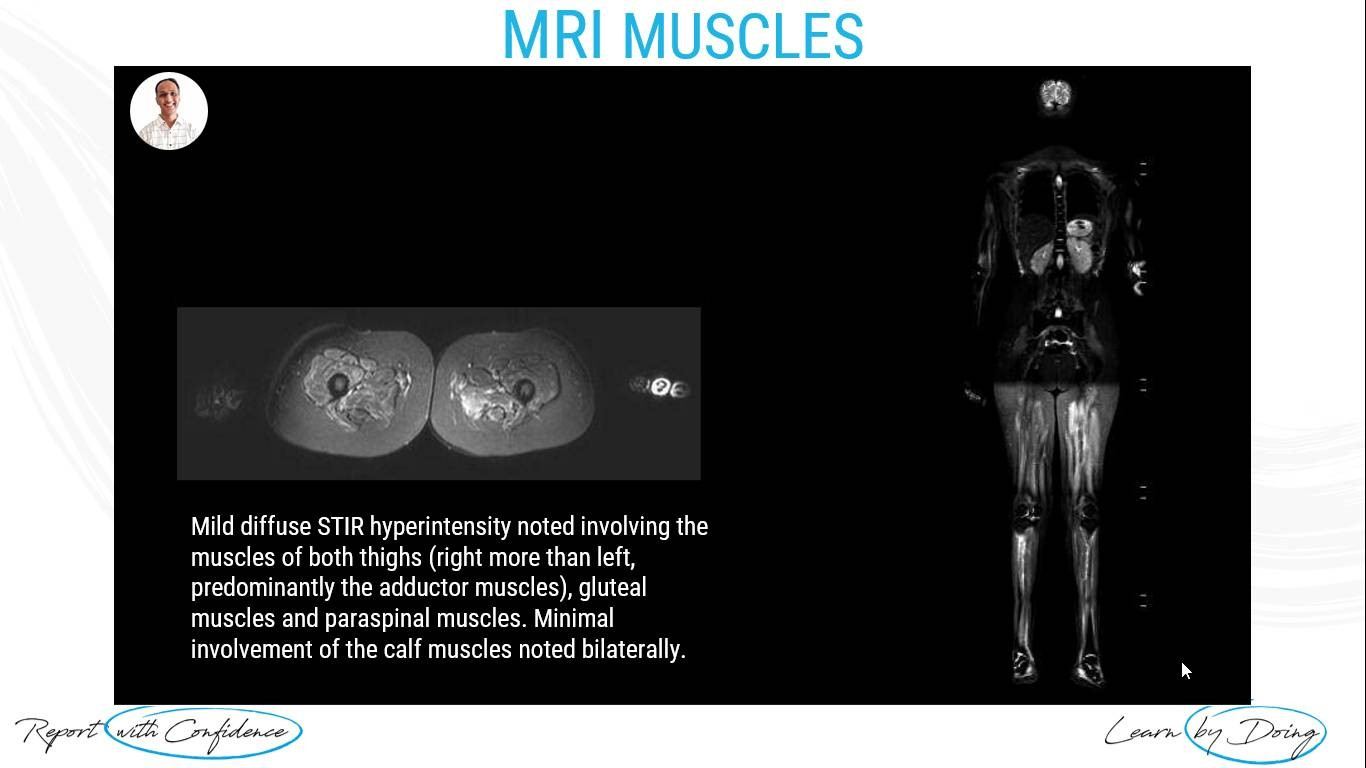
Mild diffuse STIR hyperintensity noted involving the muscles of both thighs (right more than left, predominantly the adductor muscles), gluteal muscles and paraspinal muscles. Minimal involvement of the calf muscles noted bilaterally.
![]()
- USG guided Muscle biopsy done suggestive of inflammatory myositis.
- Surprisingly CPK and other work up for myositis was negative.
- There was worsening mononeuritis multiplex.
- In spite of repeat pulse steroids, her chest pain, cardiac function and cardiac enzymes worsened.
![]()
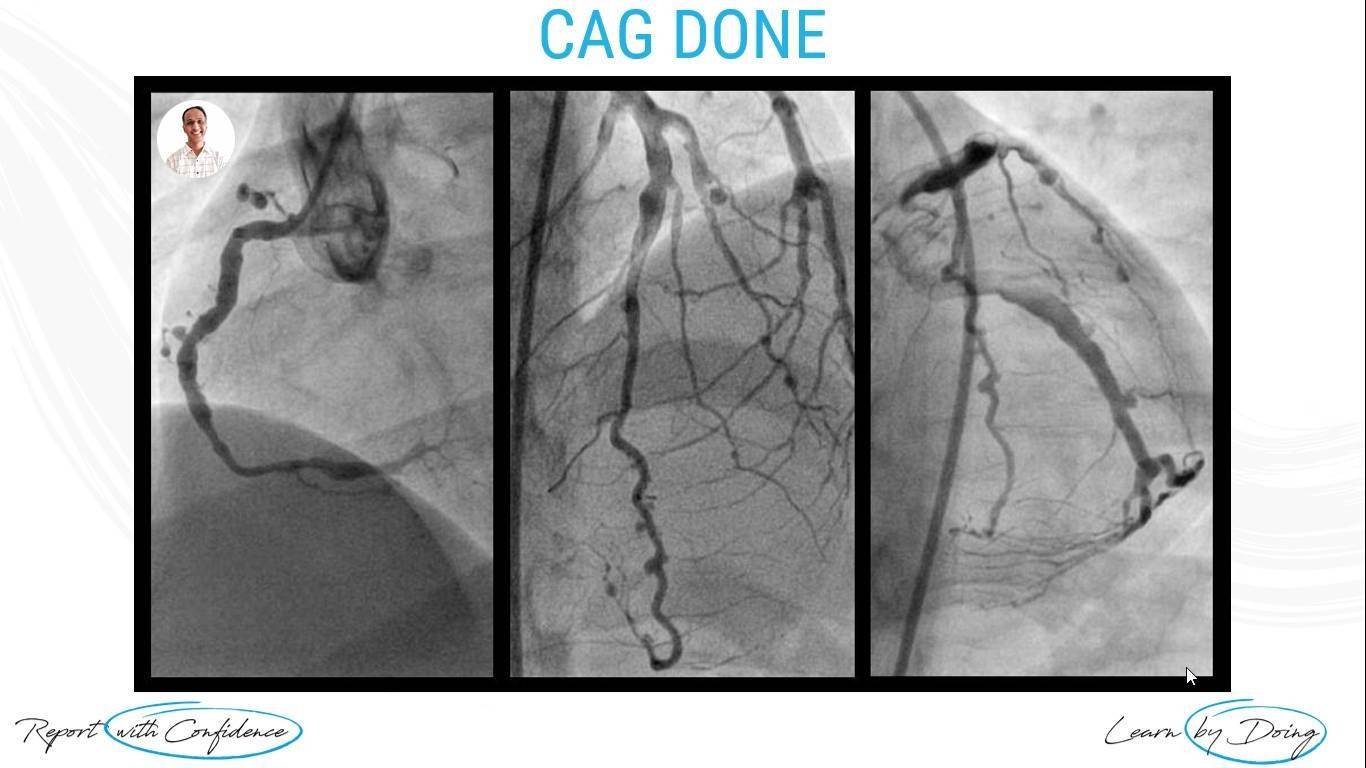
CORONARY ARTERY ANGIOGRAPHY (CAG) RESULTS:
Ectasia with multiple aneurysms distal diffuse disease (RCA - proximal ectasia with multiple aneurysms; PDA and PLV diffusely narrowed and LAD - Type III, proximal ectasia with multiple aneurysms; Ectasia of LCX) consistent with PAN.
![]()
Polyarteritis Nodosa With Myopericarditis.
![]()
- In this case clinical phenotype was that of PAN rather than lupus inspite of initial autoantibody profile, (main clue was >CRP 100).
- In a patient with myalgia/no muscle weakness and MRI suggestive of myositis, with normal CPK, think of PAN.
- Work up for DADA2 and another genetic syndrome were negative. The patient stabilized with combination of medications (Steroids + IVIG + Tofacitnib + Methotrexate).
![]()




#radedasia #mri #mskmri #radiología